Introduction
For years, risk adjustment followed a predictable playbook: meet deadlines, prepare for annual RADV, and repeat. The new MA RADV audit cycles have rewritten that playbook entirely.
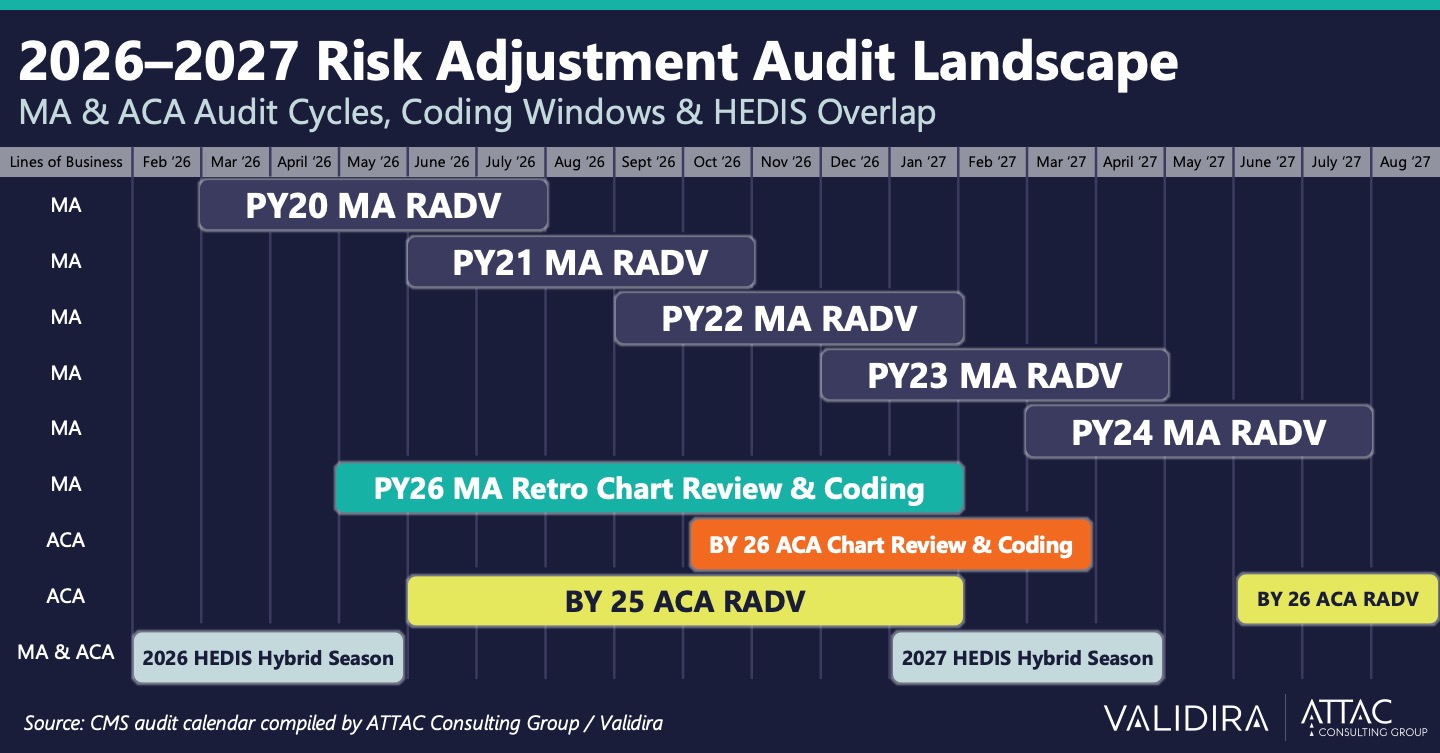
In 2026, health plans are simultaneously managing five overlapping MA RADV audit cycles — Payment Years 2020 through 2024 — while ACA risk adjustment deadline and HHS RADV audits run concurrently. Now add HEDIS hybrid seasons bookending both years, retro coding windows threading through the middle, and the September MA submission deadline closing fast, and what you have isn’t a busy season. It’s a new operating reality.
We call it the Everlasting Audit. And if your staffing model, coding infrastructure, and audit response workflows weren’t built for it, 2026 is going to be a very difficult with severe consequences if your organization is not prepared.
What Changed: CMS’s Aggressive New RADV Audit Posture
The scale of what CMS has undertaken in the past twelve months is unlike anything the Medicare Advantage industry has seen before.
CMS has introduced a plan to complete all remaining RADV audits for Payment Years 2018 through 2024 by early 2026, deploying advanced technology systems and expanding its workforce of medical coders from 40 to approximately 2,000 (CMS). More significantly, CMS will now audit all 550 eligible Medicare Advantage contracts each year, up from a previous average of 60, and has increased the number of records reviewed per plan from approximately 35 to up to 200.
New audits are now being initiated approximately every three months, starting in February 2026 with Payment Year 2020. That cadence alone fundamentally changes the planning horizon for every MA organization in the country.
For ACA plans, the picture is equally demanding. Benefit Year (BY) 25 ACA RADV is underway, BY 25 ACA Chart Review and Coding is running concurrently, and BY 26 ACA RADV follows close behind. The graphic below shows the full scope of what overlapping compliance obligations look like mapped against a single calendar.
This isn’t a busy quarter. This is the new baseline.
A Note on Extrapolation: What the September 2025 Court Ruling Means
No discussion of the current RADV landscape is complete without addressing the September 2025 federal court ruling that vacated the extrapolation provisions of the 2023 RADV Final Rule.
A federal district court vacated the RADV final rule that would have enabled CMS to extrapolate audit results across a contract’s entire population, a methodology that could have resulted in tens of millions of dollars in overpayment recoveries from a single contract (Groom Law Group).
This is a meaningful relief for MA organizations. However, it would be a serious mistake to interpret this ruling as a signal to relax audit readiness. Even without extrapolation, a 200-enrollee sample with significant unsupported diagnoses creates meaningful repayment demands, and CMS has committed to completing its backlog of audits through PY 2024 regardless of the Final Rule of litigation.
The audit cadence isn’t slowing down. The record sample sizes aren’t shrinking. And the financial and operational stakes, even without extrapolation, remain substantial for any plan with documentation gaps.
The Real Risk: What Permanent Overlap Does to Coding Quality
The financial exposure from RADV audits is well understood. What gets less attention is what permanent audit overlap does to the people and systems responsible for coding accuracy.
Laura Breisch, a risk adjustment and coding operations executive with 20+ years of experience building programs at organizations including Oscar and Datavant, put it plainly:
“In 20+ years, I’ve never seen a calendar like this one. It’s not one pressure point. It’s all of them. At once.”
When coding teams are expected to context-switch continuously between MA and ACA frameworks, with different risk models, different documentation standards, and different submission requirements, without the right infrastructure and validation layers in place, three things happen quietly:
- HCC capture rates drop. Not dramatically. Just enough to matter and impact bottom line.
- Coding decisions that were clinically supportable become harder to defend under audit scrutiny.
- Submission windows close before anyone realizes the gap.
Every supported HCC matters. Not just for revenue, but for accuracy, compliance, and defensibility when CMS comes looking. The old model of retrospective risk management is no longer sustainable. Proactive coding practices are essential for navigating this new reality.
From Episodic Readiness to Standing Infrastructure
Subbu Ramalingam, Managing Director and Practice Leader at ATTAC Consulting Group, framed the challenge this way:
“RADV readiness and coding oversight can’t be episodic. They have to be built as standing infrastructure. That means continuous operational discipline, tight retrieval and coding workflows, targeted coding validation, not random review, and clear ownership across compliance, coding, network, finance, and operations.”
The plans navigating 2026 successfully aren’t working harder than their peers. They’ve made a structural decision about what to own internally and what to bring a partner in for. Specifically, they’ve recognized that audit response capacity, coding depth, and IVA expertise are not functions that can be reliably surged from a standing start every quarter.
That’s a fundamentally different operating model than what most health plans built their teams around. And it’s the model that the Everlasting Audit demands.
What Validira Brings to the Everlasting RADV Audit
ATTAC’s Validira division was built for exactly this environment. With 20 years of risk adjustment experience spanning MA and ACA programs, Validira supported 10% of all H-contracts in the last MA RADV round. Our coding teams find 8–10% more HCCs on average than prior coding efforts, not by working faster, but by bringing the clinical depth and validation infrastructure to work across both programs simultaneously without sacrificing accuracy in either.
As one of the nation’s leading HHS RADV auditors, Validira brings the credibility and track record that matters when regulators are in the room. Our services across this landscape include:
MA & ACA RADV Audit Defense: Audit management protecting MA plans from overpayment risk and defending ACA books against HHS transfer payment adjustments.
Retrospective HCC Coding: Coding with the clinical evidence and validation layers to support every code under audit scrutiny.
Initial Validation Auditor (IVA) Services: IVA expertise that regulators recognize and respect, ensuring your data is defensible before it’s ever challenged.
Is Your Team Built for the Everlasting RADV Audit?
The 2026–2027 audit landscape isn’t a problem you can solve by asking your team to do more with less. It requires a permanent readiness posture, the kind that only comes from treating coding and audit response as standing infrastructure rather than seasonal surges.
If your team is feeling the weight of this overlap, we’d welcome a conversation about where Validira can help.
About Validira Validira is ATTAC Consulting Group’s Risk Adjustment and Coding division, providing RADV management, HCC coding, IVA services, and HEDIS hybrid support for Medicare Advantage and ACA health plans nationwide. With 20 years of experience and a track record supporting 10% of all H-contracts in the last MA RADV round, Validira brings the depth, scale, and regulatory credibility that the Forever Audit demands.

